Thyroid Gland Function in Bodybuilding | Use of Thyroid Hormones
At which Point to Drugs Truly Affect your Overall Performance Output as an Athlete?
The misconception regarding thyroid activity has been amplified by the various ads everywhere of people going on a very low-calorie diet and then supplementing with an ephedrine/caffeine combo along
with the latest thyroid booster and suddenly losing weight not necessarily fat, but body-weight. My question is "Was the loss strictly fat loss, or was there some lean body mass loss as well?" I have
a tendency to go with the latter scenario.
Now the problem is compounded in our world of pharmaceutical enhancement. Most bodybuilders have access to a wide range of drugs that are purported to help shed those extra pounds. We aren't dealing
just with creatine and guggul lipids, are we? No, we deal with growth hormone, clenbuterol. various testosterone esters, and of course T3. among others. T3 is a drug that must be taken with caution.
If you don't know how or when to use it, T3 can permanently shut down your thyroid and you can end up on thyroid medication the rest of your life. It can also be potentially life threatening in rare
cases because of its effect on the heart.
I want the reader to understand this is neither a scare-lactic article nor an endorsement. I am approaching this subject from an objective angle with the intent to educate and clear up this very
misunderstood aspect of fat loss. 1 will discuss the function of the thyroid gland, the hormones, and how to manipulate them through nutritional methods with resorting to use of T3. Too many individuals
automatically turn to T3 from the very beginning of their diet, not having the slightest clue as to how well their thyroid gland is functioning to begin with. They treat it as if it were as harmless as
caffeine. Go visit any discussion board on the Internet and my point will be proved within seconds. Look at a thread about fat loss and barn! "Use T3" is the answer. And the reasoning? "Well, it worked
for me. The weight just melted off!" Exactly. There is that word weight again. I hope that by the end of this article the reader will have a better under-standing of the function of the thyroid hormones
in the body and encourage him/her to check out the studies and articles cited for more information. Armed with this knowledge one should be able to make a prudent choice of whether or not to use T3.
PHYSIOLOGY
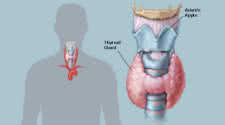
The thyroid gland is located at the top of the neck by the larynx. It stores two hormones, T4 or thyroxine and T3 or triiodothyronine. We'll just refer to them as T4 and T3 respectively. The hormones are made from iodine and tyrosine. Therefore people with inadequate intake of iodine could have thyroid problems. I would not worry about this possibility since the US adds iodine to salt. When the levels of these hormones are low the hypothalamus releases a peptide hormone called thyroid-releasing hormone (TRH), which in turn travels to the anterior pituitary and causes the release of thyrotropin (TSH). TSH then goes to the thyroid gland and tells it to produce and release thyroid hormones. Approximately 80 percent of the hormone released is T4, with the remaining being T3. T4 and T3 are very highly bound, about 99.95 percent. This state renders most of it physiologically inactive. Only about .05 percent is physiologically active and termed free. The resultant storage pool of hormones can last two to three months in the case of T4. The hormones are regulated by a simple negative feedback mechanism. The more free T3 and free T4 in the blood, the less TSH is released. Conversely the less free T3 and free T4 in the blood, the more TSH is released. The process sounds pretty simple, right? Well, now it's time to tackle the real stuff.EFFECTS OF T3 FOR THE ATHLETE
Since only 20 percent of the total amount of thyroid hormone secreted is in the form of T3, most of the T3 in our blood is converted in the peripheral tissues such as the liver, heart, kidney, muscles and the central nervous system. This conversion is important because T3 is the active thyroid hormone. It causes the physiological effects that are so sought after such as determining the basal metabolic rate. Effects on the heart and the temperature of the body result. The higher one's T3 level the faster the metabolism and therefore the higher the body temperature will be. Hence the reasoning behind taking one's temperature first thing in the morning. This practice will establish a normal temperature. During a period of dieting you'll be able to tell the thyroid is down-regulating because, among other signs, the morning temperature reading will drop. Of course this is only a rough indicator. To really see what's going on requires a blood test. If one has suspicions about the health status of one's thyroid, the morning temperature reading can be a sign of a problem. However, you must establish a normal temperature before starting the diet in order to determine what is going on. Do not simply take your temperature while dieting, see it is 97.9 degrees, and then run out and start popping T3. A temperature of 97.9 degrees may be perfectly normal for you. Everybody is different.The thyroid hormones, particularly T3, are not only catabolic but also anabolic. A weak level of T3 is mostly anabolic to muscle tissue, but as the level of T3 rises the catabolic action begins to dominate. Whether the thyroid hormones are catabolic or anabolic is determined to a large extent by the amount of insulin in the body (more on this later). The thyroid hormones also increase the number of beta receptors (i.e. good receptors) in the muscle and fat cells. This increase would allow one to build more muscle and lose more fat, since the action of epinephrine and norepinephrine, both of which work by stimulating the beta receptors, has lipolytic properties on the fat cells. If one were to block these beta receptors, however, the increase of T3 would cause the body to break down muscle tissue for energy, instead of fat, as a result of the increased energy demands of a high T3 level. This sequence illustrates why optimizing the thyroid is so important instead of just attempting to increase T3 as high as possible.
Many women suffer from hypothyroidism. That's why they always seem to be so damn cold when a man will be sweating his ass off. Apparently the major serum-binding protein for T4, TBG, is synthesized by the liver under the influence of estrogen. On paper this increase in TBG does not affect the total T4 level. However, since women have higher estrogen levels than men, more of their T4 will be bound and therefore cannot be converted to the active T3. This hypothesis has not been documented, but is simply drawn from logic on my part. Now would taking androgens that aromatize easily to estrogen affect the amount of free T4? Luckily androgens have been shown to cause a decrease in TBG concentration, which on paper does not affect the level of T4.
DIETING AND THE EFFECT ON T3
Most people realize that when one diets eventually the fat loss begins to slow down, way down, sometimes to the point of being nonexistent. The diet started great, everything was done right, but still the fat is not coming off as it did in those first few weeks. What's going on here? Several processes occur during a diet. Ideally the amount of free fatty acids mobilized increases. This increase leads to an overall loss of fat tissue. Secretion of growth hormone increases along with glucagon if you keep carbs fairly low, as is often the case. Cortisol, a catabolic hormone, increases during a period of dieting. Both insulin and insulin-like growth factor 1 (IGF-1) decrease. Last, but certainly not least, the level of free T3 in the body is also reduced through several mechanisms involving these hormones. This condition is usually referred to as euthyroid sick syndrome, where the levels of both TSH and T4 are fine, but the level of free T3 is low.Tests have shown that dieting and stressors both lower the level of free T3 in the body. During an eight-week army ranger course two groups of men were put on a diet while simultaneously enduring a sustained workload, inadequate sleep and thermal strain. (Hmm, sounds strikingly similar to dieting for a bodybuilding competition.) After the eight weeks the men's T3 was below normal, testosterone approached castration level, and IGF-1 was cut in half. Free T3 and testosterone were lowered even more by an increase of their specific binding proteins in response to a declining level of insulin. After they returned to normal feeding, the levels of all three hormones returned to normal, even while sustaining the stressors of the ranger course. Why did these levels fall?
When one's body is under stress - such as from dieting and intense training-the levels of catabolic hormones (glucagon and Cortisol) rise, while the levels of insulin and other anabolic hormones fall. The body begins to mobilize fat for energy, but only up to a point. When one has lost a specific amount of weight during a diet, the body begins a defense mechanism to stop the loss of more body mass. (This defense mechanism seems to be genetically determined through a set bodyweight point system.) In particular it tries to hold onto the muscle mass. So the body atrophies the thyroid gland and down-regulates T3 into a hormone called reverse T3, which is physiologically inactive. Another cause of the decrease in T3 is an increase of thyroxine-binding globulin during the diet. All this process acts to protect the muscle mass and organ function of the individual from being catabolized. But what do most athletes do when their weight loss has halted? Yep, they add T3! And sure as hell the weight loss resumes, at the cost of lean body mass (read muscle!). Doesn't sound so simple now, does it?
In another study nine men and five women were given either 50 mcg of T3 or a placebo for 28 days of bed rest. Serum T3 and TSH were measured before and after. After the 28 days the T3-treated group showed a twofold increase in levels of the hormone, while TSH was depressed. Most significantly the T3-treated subjects showed a greater negative nitrogen balance, lost more weight and lean body mass (read muscle!). Remember all this happened without any stress at all. These people just lay around all day. Imagine what would have happened if they were actually dieting and training without drugs. The effect of a reasonable amount of weight training would have been interesting in terms of sparing lean body mass. Would they have maintained their muscle, gained more, or lost even more? We'll have to wait for the answer to that. Or will we?
Throughout the years bodybuilders have been real, live, scientific experiments on how well a certain drug works or doesn't work. Why do some people rave about the effects of T3 without any side effects, while others damn it and end up having to medicate themselves for the rest of their lives? Well, the answer lies in the fact that most people's thyroid does not operate optimally in the first place. For those persons T3 seems like a godsend. Their diet was not working - neither was clen or GH (more on this later) -but when they add in T3 the magic started ... apparently. Others go on T3 and start losing an absurd amount of weight (damn that word!) and end up looking more like a marathon runner than a bodybuilder.
The deiodinating enzymes convert T4 to T3 in the peripheral tissues. Deiodinating enzyme II makes this conversion in the hypothalamus. During a short-term fast this enzyme is elevated and will cause a local elevation of T3. This increase in turn causes the hypothalamus to think the body is in hyperthyroidism. Therefore it suppresses the release of TRH (which causes TSH release in the pituitary). Thus we have yet another way the body fights for homeostasis.
THE UNCOUPLING PROTEINS
In the human body adenosine triphosphate (ATP) is the energy substance that powers all activities. It powers the heart, lungs and skeletal muscles. The body makes ATP from the nutrients that one consumes daily-fats, carbs and protein. To make ATP it must add a phosphate group to adenosine diphosphate (ADP). This process is called oxidative phosphorylation. The uncoupling proteins make this procedure more difficult, causing excess heat to be thrown off, hence thermo-genesis. Making ATP takes more energy than it should.There are three different types of uncoupling proteins. Uncoupling protein-1 is expressed exclusively in brown adipocytes (BAT), while uncoupling protein-2 is found widely throughout the body. Uncoupling protein-3 (UCP-3) is distinguished from the other two by its abundance in human skeletal muscle. This supply makes muscle a major site for thermogenesis in humans. The thyroid hormones increase the number of UCP-3 in the muscle cells.
In a 1997 study researchers found that in hypothyroid patients UCP-3 decreased threefold. Conversely, in hyperthyroid patients UCP-3 increased sixfold." Therefore UCP-3 may explain the effect of thyroid hormone on thermogenesis. In the same study scientists found that during starvation muscle UCP-3 increased, but BAT UCP-3 decreased. The authors suggested muscle is a major regulator of thermogenesis during starvation. This conclusion means the more muscle one has, the more fat one will burn through the thermogenic properties of UCP-3.
GROWTH HORMONE AND T3
In this age of pharmaceutical enhancement growth hormone (GH) is a common item found in the arsenal of most serious bodybuilders. In fact, it is one of the reasons why the athletes of today are so much bigger than the athletes of yesteryear. We will not consider all the effects of GH here, just the ones that affect T3. The thyroid hormones increase the number of GH receptors in the liver and they are also essential for the production of IGF-1. With an adequate number of calories GH seems to increase T3, one of the reasons GH mobilizes fat stores and increases metabolism. You'd expect that adding GH to a stack during a diet would also elevate levels of free T3, but this is not the case. A recent study showed food deprivation raised GH but depressed levels of GH-dependent variables such as IGF-1 and T3. Without IGF-1 GH does not do its magic, since it is supposed to be the mechanism by which GH exerts its effects. Therefore during a diet GH is actually catabolic. (Note that in the above study the levels of the hormones affected during fasting returned to normal after feeding.)BRING ON THE INSULIN
The pancreas releases insulin in response to a rise of sugar in the blood. It then shuttles the nutrients to their proper place. Depending on insulin sensitivity and other factors, it will go to either the muscle cells or the fat cells-we hope the former. Insulin also plays a role in thyroid function. In the presence of insulin TSH is able to stimulate the thyroid to secrete its hormones, but without it TSH will not be able to do its job. In a study scientists did with primary culture of sheep thyroid cells they found TSH, insulin and IGF-1 all interact with one another in order for the thyroid to function properly. During most diets insulin secretion is low, or should be low because of a decrease in the consumption of carbohydrates. This reduction lowers IGF-1 as well. Combined, these factors inhibit the thyroid gland from functioning optimally. Researchers have also demonstrated that a thyroid deficiency depresses levels of IGF-1 in skeletal muscle in neonatal rats. This discovery indicates that hypothyroidism will limit muscle growth. Add to that conclusion the fact that glucagon and Cortisol, both catabolic hormones, are elevated during a diet, and you realize they too inhibit thyroid function. All this evidence paints a pretty grim picture. What to do? What to do?TRIAC TO THE RESCUE?
During a diet the body scrambles to save lean body mass through several mechanisms. One is to transform thyroid hormones into reverse T3, rendering it inactive. Triac is a metabolite of T3. T3 is converted to reverse T3 in a step-by-step process. During one of these steps the body produces triac. For some reason bodybuilders began taking triac in an attempt to shed more bodyfat. It was easily available and developed a kind of cult following. (You know how the hype goes: "European pill helps burn fat!") Since triac supplementation originated in France, American bodybuilders figured they were missing out on something. If they had known the truth, triac would have been one of the last products they would have taken.Triac is not intended for people wishing to reduce fat stores because research has shown it to have weak metabolic actions in the peripheral tissues. It has a stronger binding affinity for the T3 receptors than T3, but stays there only half as long. Tests have also demonstrated triac is more potent than T3 or T4 in suppressing TSH secretion. It is very weak in promoting fat loss, but does an excellent job of slowing the metabolism through its action on TSH. If we could somehow prevent T3 from converting to triac, we could lose fat faster. This notice brings back the question of whether T3 should be elevated during a diet. In another study triac did not affect the metabolism, but it did double the amount of sex hormone-binding globulin. The effect would theoretically result in less free testosterone in the blood. For patients with a disease, such as cancer of the thyroid gland, triac works great to reduce the size of the gland through its suppressing effect on TSH secretion. Bottom line: Skip the triac.
CLENBUTEROL
Clenbuterol is a specific beta 2 agonist that has seemed to work minor miracles for about two weeks. After this period clenbuterol stops working. Unlike ephedrine, which is a nonspecific beta 2 agonist, clenbuterol fits almost perfectly into the receptor site and does not need sympathetic (adrenaline and noradrenaline) activity to do its job. Since it creates an intense stimulation of the receptor site, the body burns fat at an incredible rate. Unfortunately our bodies are well adapted to keeping us in homeostasis. After continuous use the beta 2's become desensitized to the effects of the agonist. Homologous desensitization will cause the receptors to burrow themselves into the cell so that the agonist cannot connect with them. After that, heterologous desensitization will phosphorylate the receptor, making it inactive. Moreover, after chronic supplementation clenbuterol will replace the body's own beta agonist, adrenaline and noradrenaline. So when you stop taking clenbuterol, they basically crash. No free lunch here. Now back to T3. Experiments have shown that for clenbuterol to have a positive effect on body composition the thyroid levels must be optimal. The explanation is simple. Since T3 increases the number of beta receptors on the fat and muscle cells and clenbuterol is a beta agonist, T3 will obviously increase the number of sites to work on. T3 sensitizes the beta receptors and improves the effects of clenbuterol. Sounds great, right? Well, clenbuterol will also cause the body to reduce the level of free T3, probably by lowering the conversion rate in the peripheral tissues of T4 to T3. (As a side note, phosphates have demonstrated their ability to keep the level of T3 from falling during a low-calorie diet, with a resultant increase in resting metabolic rate. The authors concluded phosphates influenced the peripheral conversion of T4 to T3 positively. Whether this process would keep the level of T3 stable during clenbuterol supplementation remains to be seen.)EPHEDRINE
Ephedrine is a nonselective beta agonist. This means it does not act directly with the beta receptors themselves, but instead requires the presence of noradrenaline to do its job. It also exhibits a generalized effect because noradrenaline can bind with both beta and alpha receptors throughout the body. Unlike clenbuterol, whose half-life is about 35 hours, ephedrine has a relatively short half-life of about four hours. These characteristics make ephedrine less potent than clenbuterol in the short term, but more potent in the long term. Since it is not as strong as clenbuterol, ephedrine does not burn out the beta 2 receptors as quickly. Chronic usage enhances the thermogenic effects of ephedrine. Contrary to clenbuterol, tests have proven ephedrine causes an increase in the ratio of T3 to T4 after four weeks on chronic supplementation. In the same study this ratio decreased below initial values after 12 weeks of chronic treatment.PLAN OF ATTACK
Now it's time to put all this information into practical use. The reader should understand that if one diets correctly for fat loss, use of T3, or any metabolite of thyroid hormone, is unnecessary, depending on the thyroid status of the subject to begin with. If you have a difficult time losing fat, a constantly low body temperature, lethargy, poor memory, no appetite or bowel irregularities, you may have hypothyroidism. On the other hand, if you have tremors, constant sweating, a voracious appetite or drastic weight loss, you may have hyperthyroidism. If you are experiencing any of these characteristics, or a combination of them, you should have your TSH, T4 and free T3 tested. Only by getting a blood test done can you know exactly what is going on. Most doctors do not like to have all three tests done, but you need to push for all three. Since many athletes experience euthyroid sick syndrome, where TSH and T4 are normal, but free T3 is low, having all three is essential. If you do have a thyroid problem, the doctor can prescribe medication to correct it. Remember, you want to optimize thyroid output, not raise it as high as possible. As the reader should know by this point, raising T3 above optimal will only cause excessive muscle-wasting.Once the thyroid output is optimal, you're ready to attack fat loss from all angles. Low-carb diets are the most effective for most people to follow. However, from the abovementioned studies we have learned that maintaining a low level of insulin for a prolonged period of time along with strenuous training will cause a decrease of T3, along with a substantial drop in testosterone (important for the natural athlete). These diets also cause Cortisol and glucagon to rise. The take-home message: No matter what kind of diet you choose to follow, be sure to interrupt it with approximately 24 to 48 hours of high-carb eating and rest (as recommended in BodyOpus) once every 7 to 10 days. You can determine the frequency of this high-carb fest by individual factors such as whether you're a natural or pharmaceutical enhanced bodybuilder and whether you are behind or ahead of schedule. We know this type of refeeding increases T3, insulin, IGF and testosterone while decreasing the catabolic hormones Cortisol and glucagon. An example of this schedule would be dieting and training Monday to Friday and then taking Saturday and Sunday off training and dieting to carb up, stabilize the anabolic hormones, and grow. The individual bodybuilder must find out what works best for him by experimenting with the amount of time dieting and the length of the rest and carb-up. The main point is to use this information to lose the most fat without losing muscle and without automatically resorting to T3.
Give yourself plenty of time to lose the fat. If you have 20 pounds of fat to lose for a contest, do not try to lose it in four weeks. Overtraining is also a cause of thyroid slowdown, so attempting to shed those extra pounds through excessive cardio and weight training is a no-no. Staying lean in the offseason is the best approach. This way you won't have to lose an excessive amount of fat precontest and therefore will not lose muscle in the process. Nothing is more depressing than working hard to build up a large amount of muscle, only to lose it while dieting.
Use thermogenics such as the ephedrine/caffeine combo, which has proven itself safe over the years, spares muscle while dieting, improves with chronic use, and actually raises thyroid hormone levels after four weeks of continuous use. Since the ratio of T3 to T4 drops below initial levels after 12 weeks of continuous use, using it only 8 to 10 weeks should prevent the thyroid from slowing down. The e/c stack works better the longer you use it, so the question of whether you'd be better off starting it at the outset of your diet or saving it for the final weeks remains to be conclusively answered.
If you decide to go the clenbuterol route, have a doctor check your thyroid level before and after two weeks of usage. Since the thyroid level will almost certainly be lower after, you could try supplementing with phosphates to see if that makes a difference in keeping the level stable. Using ephedrine/ caffeine for eight weeks before hitting clen may increase the number of beta receptors through its elevation of T3, on which clen exerts its effects. Remember, also, that clenbuterol seems to work only the first time for most users. After that it becomes close to useless. This evaluation assumes the bodybuilder uses no supplemental T3.
For those trainers who still wish to use T3, this is what you should do. First, of course, get your levels checked. If the levels are low, ask the doctor for a prescription. (Even if they are in the low normal range, you probably won't get a prescription.) If you want to take matters into your own hands, obtain a copy of the test results and find out where the levels are. The normal range should appear directly across from the drawn values. If the free T3 is low, begin by taking one 25-mcg tablet daily. Wait one week and have the levels drawn again. If you're losing fat and the levels are higher, leave the dosage alone. Do not increase it further. Increasing it will only exacerbate muscle-wasting. If you're not losing fat and the levels have not moved appreciably, increase the dosage to 50 mcg (which equates to two 25-mcg tabs) a day, and check again. Continue this pattern until you're losing a perceptible amount of fat without losing muscle. If you are unsure, the golden rule here is, more is definitely not better. Experts have various views as to how long one can safely use T3 without shutting the thyroid down permanently. Some say four weeks, others six, others eight. The only recommendation they all have in common is that one should taper usage down, just as it was tapered up. Do not just stop abruptly unless you like the soft, bloated look. Taking in any amount of exogenous T3 will sup-press TSH secretion, but how far one can push it without risking permanent shutdown is open to debate.
Is having the blood levels drawn absolutely necessary? If you don't want to run the risk of permanently messing up your thyroid gland and losing muscle, yes it is! Of course, not everyone will follow this recommendation. Just remember, you have been warned. Two final rules: Do not use T3 without the aid of anabolics and do not use T4 (L-thyroxin, Synthroid). Using T4 would be a colossal waste of time for most dieters because the problem usually lies in a faulty conversion of T3 to T4 in the peripheral tissues. Using T4 will only cause TSH suppression and a subsequent crash.
CONCLUSION
I hope that this article has enlightened the reader about the implications of taking T3. In the continuous struggle to reduce body-fat and build muscle, some bodybuilders choose to take a more radical and aggressive approach. This does not make it bad or wrong necessarily, just as long as the person understands all the potential consequences of his/her actions. Truth be told, we don't know exactly how much or how long supple-mental T3 can be taken without causing permanent adverse effects. Some people have taken supplemental T3 for months - and in some cases years-with seemingly little or no side effect. I have stated some of the reasons, but many questions still remain to be answered.As we learn more about the effects of diet and training on hormonal status, we realize these are the greatest tools available in manipulating body composition. This is where most study should focus in the future. Such research will benefit all of us chemically enhanced and naturals alike.